
MX3 CMO Prof. Trevor Kilpatrick presented at the Minesafe International 2020 Conference. Trevor’s talk detailed the importance of heat stress and hydration management on the worksite and compared the scientific evidence behind the different technologies available for workplace hydration assessment, including the MX3 Hydration Testing System.
Minesafe is the premiere Australian mining safety conference and is attended by a diverse audience of mining regulators, health and safety practitioners and other resource industry professionals.
“We are on the cusp of a revolution in workplace safety driven by technology.”
This article is adapted from Prof Trevor Kilpatrick’s presentation at Minesafe 2020.
Heat Stress and Hydration Management – Evidence, Technologies and Biomarkers
Work-related heat stress is a major issue in Australia.

Between 2000 and 2015, 17 heat-related deaths were reported on Australian worksites1. The true influence of heat stress on fatalities and severe injuries is likely much greater, with heat exposure predisposing individuals to heart attacks and injury due to poor decision making induced by the cognitive disfunction associated with dehydration. Poorly managed hydration can lead to many negative outcomes, including increased fatigue, reduce physical strength, poor judgement and compromised coordination and reaction time. These effects predispose to both injury and accidents.
From an economic perspective, these outcomes result in tremendous productivity losses, amounting to close to 7 billion dollars per year in Australia, approximately 0.4% of GDP2. Some 30% of workers experience heat-related productivity loss, with many heat related injuries can result in extended absences from work3.
How can heat Strain be avoided?
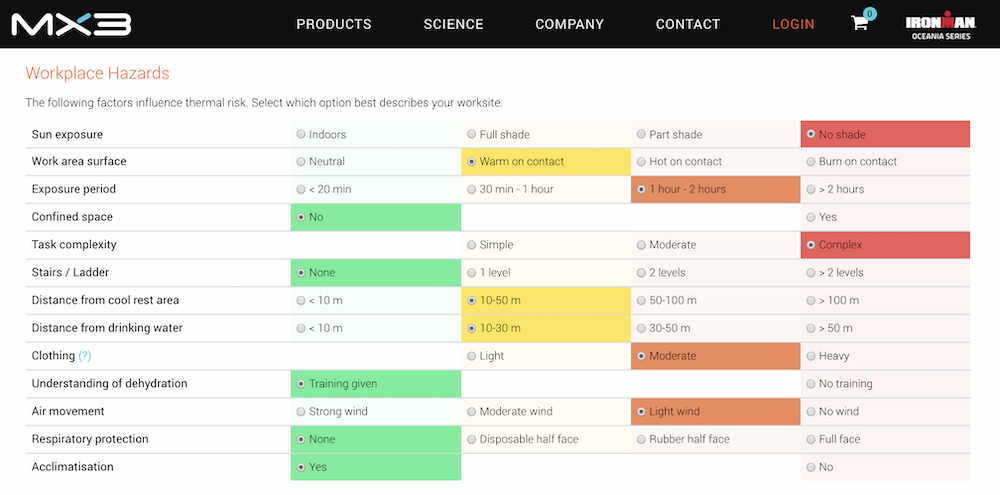
One strategy is to understand the magnitude of thermal risk related to physical and environmental conditions on a worksite with thermal risk assessment tools, such as the method described by Australian Institute of Occupational Hygienists. These tools allow a health and safety officer to quantify thermal risk and recognise appropriate controls that reduce heat strain. Another general strategy is to establish educational programs so workers can self-assess for heat strain symptoms and understand good fluid replacement habits. Where possible, a gradual and regular increase in heat expose will allow workers to acclimate to more extreme conditions and build up physical tolerance to heat stress, reducing the likelihood of injury4.
However, while workplace-level approaches are very important, they are a blunt instrument. All workers do not respond equally to heat, and there is a large amount of inter- and intra-individual variation in sweat rate and sweat composition driven by intrinsic genetic variation as well as environmental conditions, heaviness of clothing and protective equipment, work intensity, diet and degree of acclimation5. For these reasons a personalised approach to assessment of fluid loss is very much required.
How can hydration status be measured?
While there is no absolute gold standard for hydration assessment, there are many technologies which are currently employed6. Laboratory methods include isotope dilution which determine whole body water content, or plasma osmolality which describes the concentration of solutes in plasma. These methods are too complex, expensive and invasive for routine hydration assessment on the worksite. More practical methods include the assessment of body mass loss (BML), urine specific gravity (USG) or salivary osmolarity (SOSM).
Change in body mass is a good indicator of fluid loss during physical activity but a poor indicator of hydration status before activity due to day-to-day fluctuations in weight caused by diet, urination and excretion7. Nude BML measurements are most reliable, as fluid captured in clothing during exercise may lead to underestimation of fluid loss. However, this is difficult to implement for spot checks of hydration on the worksite.
“While workplace-level approaches are very important, they are a blunt instrument. A personalised approach to assessment of fluid loss is very much required.”
USG, the measure of the density of urine, is typically established from measurements with a handheld refractometer. Urine samples are unpleasant to collect and measure, and urinary spot checks are highly variable, influenced by activity, diet and fluid intake over the course of several hours. For these reasons, the most reliable and informative USG measurements are from first-morning urine8. Such samples are difficult to obtain, susceptible to manipulation and do not allow for assessment of hydration status during or after work. Several studies have now shown that USG spot checks greatly overestimate the number of individuals who are dehydrated, when compared to plasma measurements9,10.
SOSM is the measure of the concentration of particles in saliva – predominately electrolytes. Importantly, saliva sampling is non-invasive and can be conducted in a safe and sterile manner. There is an increasing body of literature demonstrating that SOSM measures are a reliable indicator of hydration status, correlating with both changes in plasma osmolarity and body mass11,12. Interestingly, SOSM was found to be the most effective ancillary tool for assessing hydration status in the elderly presenting to the emergency department when benchmarked against plasma osmolarity and kidney function13.
The MX3 Hydration Testing System is a game changer

Until recently, SOSM measurement was considered impractical due to the cost and technical complexity of laboratory osmometers, but this is now changing. Over the last 4 years MX3 has developed the MX3 Hydration Testing System (HTS) to make routine measurement of SOSM accessible and user friendly. The HTS is the world’s first real-time, electrochemical saliva testing system. It comprises a disposable sensor, which is slotted into the handheld device and then dabbed directly on to the tongue for a few seconds after which an immediate, actionable measurement is reported. I’m pleased to report that our technology has now been adopted at over 20 Australian mining sites.
”Saliva sampling is non-invasive and can be conducted in a safe and sterile manner… MX3 makes the routine measurement of SOSM accessible and user friendly.”
The rollout of the MX3 HTS to these sites has allowed us to gain some key insights into the hydration status of personnel on Australia mine sites. We have observed that a significant percentage of workers, over half, are typically mildly or moderately dehydrated when entering the workplace, and that routine measurement with the MX3 system over multiple days is associated with a gradual improvement in hydration status, potentially driven by the increased focus on hydration monitoring.
In summary, we are on the cusp of a revolution in workplace safety driven by technology to enable quantitation of relevant and actionable physiological parameters in our workers. In one important domain, the minimisation of heat stress, the measurement of SOSM using a system such as the MX3 Hydration Testing System has much to offer.
1 Gun, R. Deaths in Australia from Work-Related Heat Stress, 2000-2015. Int J Environ Res Public Health 16, doi:10.3390/ijerph16193601 (2019).
2 Zander, K. K., Botzen, W. J., Oppermann, E., Kjellstrom, T. & Garnett, S. T. Heat stress causes substantial labour productivity loss in Australia. Nature Climate Change 5, 647-651 (2015).
3 Flouris, A. D. et al. Workers’ health and productivity under occupational heat strain: a systematic review and meta-analysis. The Lancet Planetary Health 2, e521-e531 (2018).
4 Périard, J. D., Travers, G. J., Racinais, S. & Sawka, M. N. Cardiovascular adaptations supporting human exercise-heat acclimation. Autonomic Neuroscience 196, 52-62 (2016).
5 Baker, L. B., Barnes, K. A., Anderson, M. L., Passe, D. H. & Stofan, J. R. Normative data for regional sweat sodium concentration and whole-body sweating rate in athletes. J Sports Sci 34, 358-368, doi:10.1080/02640414.2015.1055291 (2016).
6 Armstrong, L. E. Assessing hydration status: the elusive gold standard. Journal of the American College of Nutrition 26, 575S-584S (2007).
7 Sawka, M. N. et al. American College of Sports Medicine position stand. Exercise and fluid replacement. Medicine and science in sports and exercise 39, 377-390 (2007).
8 Cheuvront, S. N., Kenefick, R. W. & Zambraski, E. J. Spot Urine Concentrations Should Not be Used for Hydration Assessment: A Methodology Review. Int J Sport Nutr Exerc Metab 25, 293-297, doi:10.1123/ijsnem.2014-0138 (2015).
9 Hew-Butler, T. D., Eskin, C., Bickham, J., Rusnak, M. & VanderMeulen, M. Dehydration is how you define it: comparison of 318 blood and urine athlete spot checks. BMJ Open Sport Exerc Med 4, e000297, doi:10.1136/bmjsem-2017-000297 (2018).
10 Sommerfield, L. M. et al. Validity of urine specific gravity when compared to plasma osmolality as a measure of hydration status in male and female NCAA collegiate athletes. Journal of strength and conditioning research/National Strength & Conditioning Association 30, 2219 (2016).
11 Walsh, N. P. et al. Saliva parameters as potential indices of hydration status during acute dehydration. Medicine & Science in Sports & Exercise 36, 1535-1542 (2004).
12 Muñoz, C. et al. Assessment of hydration biomarkers including salivary osmolality during passive and active dehydration. European journal of clinical nutrition 67, 1257-1263 (2013).
13 Fortes, M. B. et al. Is this elderly patient dehydrated? Diagnostic accuracy of hydration assessment using physical signs, urine, and saliva markers. Journal of the American Medical Directors Association 16, 221-228 (2015).